FRACTURES OF THE SCAPHOID
Fractures of the
scaphoid are among the most common fractures of the wrist after fractures of
the distal radius and represent the most common fracture of a carpal bone.150,393,537 The position of the scaphoid on the radial side of
the wrist, as a proximal extension of the thumb ray, makes it vulnerable to
injury. Not only does the scaphoid mechanically link the proximal and distal
carpal rows, but it is also firmly attached at both ends to strong ligament
systems that limit and control its motion.47
It is self-evident that the scaphoid flexes with wrist flexion and extends with
wrist extension, but it also flexes during radial deviation and extends with
ulnar deviation. These factors make immobilization of scaphoid fractures
difficult, especially when there is displacement. This change in position of
the scaphoid during different planes of wrist motion confirms the scaphoid's
role as the mechanistic key that controls wrist stability and serves as the
principal bony support between the proximal and distal carpal rows and for
carrying compressive loads from the hand across the wrist to the distal
forearm. There are two different mechanisms of scaphoid fracture that may
explain the differences in clinical presentation-compression injury and
hyperextension, bending injury (Fig. 12-86). The compression fracture from a
more longitudinal load or impaction of the wrist leads to intraction of the
scaphoid without displacement. Tensile stresses generated palmarly when
excessive hyperextension is applied to the wrist and when tensile forces exceed
bone strength produce a fracture through the scaphoid that commonly results in
fracture displacement. As a result of these two different mechanisms, scaphoid
fractures can present as nondisplaced, stable fractures or as displaced,
unstable fractures.138
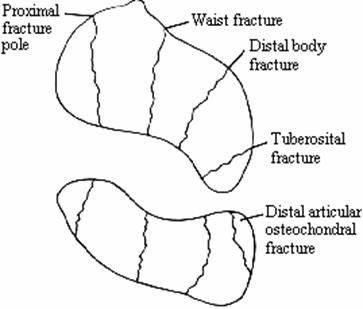
Fig. 12-86 65%-waist;
15%-proximal pole; 10%-distal body; 8%-tuberosity; 2%-distal articular surface.
The scaphoid is an irregularly
shaped bone, more resembling a deformed peanut than the boat for which it is
named. It rests in a plane at 45° to the longitudinal axis of the wrist.
Articular cartilage covers 80% of the surface. The proximal pole is constrained
to the lunate by an interosseous ligament. The distal pole has a V-shaped
scaphotrapezial ligament, a scaphocapitate ligament, and a dorsal capsule. It
rests on and can be attached along the ulnar aspect of the waist to the
radioscaphocapitate ligament. The only other capsular influence is where the
dorsal intercarpal ligament inserts obliquely on a roughened ridge and brings
the primary blood supply that enters the scaphoid. Otherwise, the scaphoid has
no ligamentous or tendinous attachments and acts with the rest of the proximal
carpal row as 'intercalated segments' subjected to the forces acting
on them.89,309 Compressive forces, acting across a three-link structure, cause
a zig-zag collapse deformity. With a scaphoid fracture, the distal scaphoid
tends to flex and the proximal scaphoid extends with the proximal carpal row.
As a consequence, angulation occurs at the fracture site, which gaps open
dorsally and gradually assumes the so-called humpback deformity.18 Studies have shown that this deformity may
occur at the time of fracture and result in immediate malposition of the
scaphoid fragments into radial as well as dorsal angulation.490 Failure to
correct such deformity leads to fracture malalignment, nonunion, or
malunion.322,342
Despite the lack of direct tendon
attachment, joint compressive forces, trapezial-scaphoid shear stress, and
capitolunate rotation moments exert control on the scaphoid. As a consequence
of these biologic and mechanical factors, scaphoid fractures have a high
incidence of nonunion (8% to 10%), frequent malunion, and late sequelae of
carpal instability and post-traumatic arthritis. Next we examine the diagnosis
and treatment of acute scaphoid fractures and address the treatment options
available when scaphoid union is either delayed or absent.
Acute Scaphoid Fractures
Acute fractures
of the scaphoid were first recognized in 1889 by Cousin and Destot145 before
the discovery of x-ray. A clear description was made later, in 1919, by Mouchet
and Jeanne.268 Scaphoid fractures are usually an injury of young men occurring
after a fall, athletic injury, or motor vehicle accident. The mechanism of
fracture is usually considered a bending fracture with compression dorsal and
tension palmar. However, axial loading compression injuries have been suggested
as another mechanism, particularly in the nondisplaced, stable fracture.256a
Scaphoid fractures in children are uncommon, because the physis of the distal
radius usually fails first.7,103,173,235,311,531
Concomitant fractures of the distal radius and scaphoid have been reported.256b,530a,531
Similarly, in the elderly, the distal radial metaphysis usually fails with
fracture before the scaphoid fractures.
The patient often presents to the
emergency department complaining of wrist pain and may be diagnosed as having a
'sprain' of the wrist. In sports injuries it is not uncommon for the
wrist injury to go unnoticed, with the request for evaluation and treatment
delayed.342 Fractures of the scaphoid in adolescents, previously believed
uncommon, are now being reported more frequently and with different clinical
appearance.377a,500a
Signs and Symptoms
The diagnosis of
a scaphoid fracture is made on clinical examination where the index of
suspicion is raised and by proper radiographic examination, by which the
diagnosis is confirmed (see Fig. 12-47B).146 Clinical examination should
demonstrate tenderness in the snuffbox region of the wrist, over the
tuberosity, or on the proximal pole of the scaphoid just distal to Lister's
tubercle. Range of motion is reduced but not dramatically. There is usually
pain at the extremes of motion. Swelling or ecchymosis is not present except in
fracture-dislocations. Clearly, these same physical findings may be present
with ligamentous injuries of the wrist, and thus whenever there are any
findings suggestive of a scaphoid fracture,124,146 the
patient should be treated for a suspected scaphoid fracture.103
Radiographic Examination
Radiographic
diagnosis of a scaphoid fracture often requires special views and occasionally
special tests.160,173,468 The emergency
posteroanterior and lateral x-rays146 should also include a scaphoid view (see
Fig. 12-22), which puts the scaphoid in profile. Motion views of the wrist
(Fig. 12-87) (flexion-extension and radial and ulnar deviation) may demonstrate
fracture displacement, which is an indication of an unstable scaphoid fracture.
These same x-rays should be repeated at 2 to 3 weeks if the initial films were
negative. It is imperative for the treating physician to make the diagnosis at
this time, because a delay in diagnosis increases the incidence of scaphoid
nonunion.160 If a diagnosis still cannot be confirmed with confidence on
routine films, a technetium bone scan (Fig. 12-88),45,202,411,417
polytomography (Fig. 12-89),58,223,403 or MRI (Fig. 12-90 and Fig. 12-91)51,261a
of the wrist is recommended, in that order of preference.222,411,417,438,525a
Ultrasonography and intrasound vibration examination have also been used to
detect the occult, undiagnosed scaphoid fracture.102,181a We have been
impressed with the ability of both CT scanning276a and MRI to clearly show a
scaphoid fracture when both plain films and even polytomography were not
diagnostic of a fracture.57,261a Most authorities recommend bone scintigraphy
as the procedure of choice for a suspected but unconfirmed
fracture.45,202,444a,525a,525b
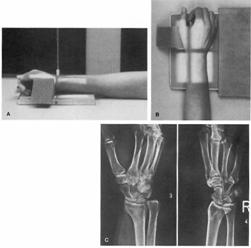
Fig.
12-22 Incidenta oblica scafoido-radiala (AP In
supinatie). A) Antebratul este asezat pe masa cu
radiocarpul asezat in centrul casetei; B) Antebratul este rotat in
pronatie de 45 grade sprijinit pe support; C) Aceasta incidenta
pune in evidenta scafoidul pe toata lungimea de profil (stg);
prin comparatie incidenta oblica ulnara arata
suprapunerea capitatului Si al semilunarului peste scafoid cu
evidentierea buna a articulatiei scafo-radiale (dr)
When instability of the scaphoid is
suspected, careful analysis of the lateral x-ray for intrascaphoid angulation
or a dorsally tilted lunate is recommended (Fig. 12-92). Motion views comparing
scaphoid position during radial and ulnar deviation may also demonstrate motion
at the fracture site (see Fig. 12-87). Polytomography, however, is a good
method to determine scaphoid displacement.51 Lateral tomography or lateral CT
(and axial) scanning can be used to measure the exact degree of intrascaphoid
angulation or displacement (see Fig. 12-92).332,468 Three-dimensional imaging
of scaphoid fractures and fracture nonunions has been reported both to assess
displacement mechanisms as well as to plan treatment.45a From biplanar
trispiral tomography, we have studied the range of normal angulation of the
scaphoid to detect displacement and instability.490,491 Measurements appear to
be reproducible to within 5° and, when compared with the uninvolved scaphoid,
provide information to assess not only the presence of displacement but the
accuracy of reduction. Three-dimensional representation of the scaphoid using
CT scanning and three-dimensional imaging provides the ability to describe
displacement in all three planes and has promising clinical application.45
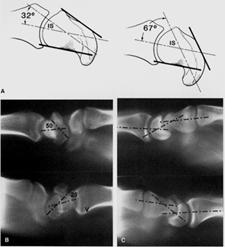
Fig. 12-92 Angularea
scafoidului. A) Scafoid normal si scafoid
cu deformare in cocoasa. Unghiul intrascafoidian (IS) lateral normal este
35+/-5 grade. B)Fractura scafoid bilaterala
cu deplasare vicios consolidata cu IS anormal de 50 (sus) si normal
de 28 (jos), in ciuda cominutiei dorsale; C) Unghiul capitulo-lunat poate
fi util in stabilirea instabilitatii fracturii: sus de 35 grade, jos
de 25 de grade. Ambele unghiuri confirma instabilitatea
carpiana asociata cu fractura de scafoid cu deplasare.
Differentiation between an acute
scaphoid fracture and a scaphoid nonunion is important for planning treatment,
and only proper x-rays can make the difference evident. Not uncommonly, a
second injury will draw attention to a minimally symptomatic nonunion
aggravated by the recent event. The acute scaphoid fracture is represented by a
single line through the bone, occasionally with dorsalradial comminution and
dorsal angulation. Late presentation of a fracture or established nonunion,
conversely, will demonstrate resorption at the fracture site (evident as a space
between the fragments), subchondral sclerosis, and displacement on both the
posteroanterior and lateral x-rays.12 A true pseudarthrosis separates delayed
acute fracture from established nonunions. The longer the period of time since
injury, the greater the cystic resorption, the denser the sclerosis, the more
prominent the shortening of the scaphoid, and the greater the loss of carpal
height. Secondary degenerative changes are usually present by
10 to 15 years.322
Classification
Fractures of the
scaphoid may be classified either by the location of the fracture within the
bone or by the amount of fracture displacement (stability).
Location
Classification
by anatomical location has many proponents, some of whom attempt to correlate
fracture union rate with the site of injury (see Fig. 12-86). Five different
fracture sites have been described: tuberosity, distal third, waist, proximal
third, and distal osteochondral fractures.116,537 All but the tuberosity
fractures are intra-articular to a greater or lesser degree.122,252,443 From a
series of scaphoid fractures carefully studied, waist fractures accounted for
80%, proximal pole, 15%; tuberosity, 4%; and distal articular, 1%. Nonunion of
the distal scaphoid has only recently been recognized and reported.384a The other anatomical classification is based on the
direction of the fracture, with horizontal, oblique, avulsion, and comminuted
types described.
The healing time
for these different fracture types ranges from 4 to 6 weeks for tuberosity
fractures, 10 to 12 weeks for distal third and waist fractures, and 12 to 20
weeks for proximal pole fractures.
The blood supply of the scaphoid is
critical in regard to fracture location. Gelberman's work214 confirmed earlier
studies demonstrating that the major blood supply
comes from the scaphoid branches of the radial artery, entering the dorsal
ridge and supplying 70% to 80% of the bone, including the proximal pole. The
second major group of vessels enters the scaphoid tubercle, perfusing only the
distal 30% of the bone. With fractures through the waist and proximal third,
revascularization will occur only with fracture healing. One can assume that
with proper treatment nearly 100% of tuberosity and distal third scaphoid will
heal; 80% to 90% of fractures at the waist will heal; and only 60% to 70% of
proximal pole fractures will heal. Similarly, oblique or shear fractures have
been shown to have delayed healing in comparison to horizontal fractures.
Comminuted or distracted osteochrondral fractures will have the poorest rate of
union.
Stability
 The second major classification of scaphoid fractures subdivides
them into either stable or unstable fractures.116,252
A stable fracture is one that is nondisplaced, and it may have an intact
cartilage envelope. That is, the fracture may occur within the bony substance
of the scaphoid, usually from an impaction rather than a bending mechanism,
incompletely separating the two fracture components. X-rays in two planes, as
well as motion views, do not show any step-off or displacement of these
fractures. The unstable scaphoid fracture, conversely, is by definition
displaced with a step-off of 1 mm or more of angulation of the scaphoid in a
lateral x-ray (Fig. 12-93). Rotational displacement can also be detected. The
rate of fracture union and options for treatment change dramatically when one
compares unstable and stable scaphoid fractures. Unstable fractures can be
simply displacement from bending fracture mechanisms or from high energy,
leading to fracture-dislocations of the wrist.
The second major classification of scaphoid fractures subdivides
them into either stable or unstable fractures.116,252
A stable fracture is one that is nondisplaced, and it may have an intact
cartilage envelope. That is, the fracture may occur within the bony substance
of the scaphoid, usually from an impaction rather than a bending mechanism,
incompletely separating the two fracture components. X-rays in two planes, as
well as motion views, do not show any step-off or displacement of these
fractures. The unstable scaphoid fracture, conversely, is by definition
displaced with a step-off of 1 mm or more of angulation of the scaphoid in a
lateral x-ray (Fig. 12-93). Rotational displacement can also be detected. The
rate of fracture union and options for treatment change dramatically when one
compares unstable and stable scaphoid fractures. Unstable fractures can be
simply displacement from bending fracture mechanisms or from high energy,
leading to fracture-dislocations of the wrist.
Fig.
12-93 Fractura instabila
Treatment
Nondisplaced Fractures
The primary
treatment for acute fractures of the scaphoid is cast or splint
immobilization.506,559b As mentioned earlier, when
there is any question regarding the presence of a scaphoid fracture, cast
immobilization is recommended for 2 to 3 weeks until the diagnosis can be
reassessed. The debate between long- and short-arm casts, as well as the
position of immobilization, has not been definitely answered, but findings of
recent studies should influence our decision.35a,395 In one prospective study,
Gellman and coauthors compared short- and long-thumb spica casts and noted
decreased time to union and reduced rates of delayed union and nonunion with a
long-arm thumb spica cast.217 The findings in this study agree with those of
earlier reports84,183,226,537 that noted higher rates of healing with a
long-arm cast for 4 to 6 weeks. Conversely, those surgeons who prefer a
short-arm thumb spica cast point to 95% union rates in their personal series.
Furthermore, a study from Nottingham, England, suggests that the thumb does not
need to be included, provided the wrist is immobilized in the treatment of the
acute, nondisplaced fracture.105a Tuberosity fractures are undoubtedly suitable
for a short-arm cast, while patients with proximal pole fractures are
candidates for a long-arm cast (if not open fracture treatment).
The
recommended position of immobilization for scaphoid fractures varies from full
extension to slight flexion, with varying degrees of radial or ulnar deviation.
The amount of fracture displacement, alignment in both the posteroanterior and
lateral planes, and associated injuries have been analyzed by several
biomechanical studies, suggesting that a position of neutral flexion-extension
and slight ulnar deviation is the preferred position of nondisplaced and
minimally displaced scaphoid fractures. To reduce the stress produced by the
volar and radiocapitate ligament, Weber and Chao553 recommended radial
deviation and palmar flexion. This position makes radiographic assessment
difficult. From an analysis of simulated displaced fractures
it would appear that slight radial or ulnar deviation is acceptable, along with
neutral flexion-extension. If the effect of lunate extension on dorsal gapping
of the fracture site is important, then an attempt at flexing the lunate should
help control the scaphoid reduction. This can be accomplished by careful
molding of the cast. A depression is created over the capitate neck while displacing
the carpometacarpal area relative to the forearm. The capitate tends to
derotate the lunate and proximal pole, providing better coaptation of the
fracture fragments (Fig. 12-94).
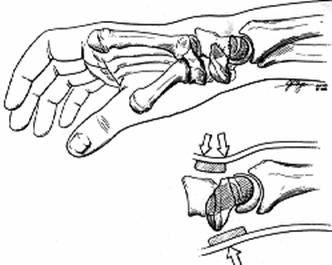
Fig. 12-94 Reducerea ortopedica a unei fracturi de scafoid cu
deplasare prin presiune in trei puncte. In sus
se apasa de pe fata palmara extremitatea distala a
scafoidului iar in jos se apasa pe fata
dorsala pe capitat si semilunar.Deplasarea capitatului palmar
roteste semilunarul si polul proximal al scafoidului in flexie
si inchide lacuna posterioara.
For nondisplaced stable scaphoid
fractures (Fig. 12-95), we recommend a long-arm thumb spica cast, with the
wrist in neutral deviation and neutral flexion-extension for 6 weeks, followed
by a short-arm thumb spica cast until there is radiographic union confirmed by
polytomography.116 The union rate should exceed 95%. Delay in recognition,
delay in initial treatment, and proximal third location of the fracture all
negatively influence fracture healing.
Displaced Fractures
Author's Preferred
Method of Treatment. Displaced fractures of the scaphoid require
treatment different from that for nondisplaced fractures. A displaced fracture,
by definition, is one with greater than 1 mm of step-off or more than 60° of
scapholunate or 15° of lunatocapitate angulation as observed on either plain
x-rays or tomography.117 The degree of instability may
vary, and thus there are different choices for fracture treatment. We believe
that there is still a role for a carefully applied long-arm thumb spica cast in
the treatment of displaced scaphoid fractures, provided that the fracture can
be acceptably reduced and the reduction maintained. To effect the reduction,
three-point pressure on the tubercle of the distal scaphoid palmarly is
combined with dorsal pressure over the capitate and dorsal support at the
distal radius, which helps reduce and maintain the dorsal lunate angulation
(see Fig. 12-94). An acceptable reduction includes alignment with less than 1
mm of displacement and a scapholunate angle of not more than 60°. With lateral
tomography (or CT scanning), lateral intrascaphoid angulation should not exceed
25° ± 5°, and the posteroanterior angulation should be not more than 35° ± 5°.
If an accurate fracture reduction
cannot be obtained, then other methods of treatment should be considered. These
include closed reduction and percutaneous pin fixation, open reduction and pin
fixation,167 and open reduction and compression screw fixation (Fig. 12-96 and
Fig. 12-97).88,140,251,253,310 For acute displaced fractures that cannot be
easily reduced, we recommend open reduction and Kirschner-wire or compression
screw fixation of the scaphoid. The technique we prefer is to realign the
proximal scaphoid and lunate to the distal radius and secure them with
Kirschner wires. The proximal fracture components are stabilized by this
procedure. The distal scaphoid can then be reduced onto the proximal fragments
and fixed in that position. In addition to Kirschner-wire fixation or
compression screw (AO, Herbert), a long-arm thumb spica cast is maintained for
6 weeks. After Kischner-wire removal, a short-arm cast is applied until
fracture healing is confirmed radiographically (preferably with polytomography
or CT scan).
Fig. 12-97 A)
Insertia unui surub de compresiune.
Reducerea cu brosa K se face inainte de introducerea surubului
(vedere din proximal spre distal (sus) si lateral-radial (jos). B) Fractura cominutiva 1/3 distala
scafoid redusa si fixata cu brosa si surub
Herbert. Corectia inclinarii dorsale a semilunarului s-a efectuat anterior de reducerea scafoidului si
fixata cu o brosa. C) Incidenta laterala a
sintezei.
With the advent of new compression
screws and staples for the scaphoid, internal fixation has become more
popular.88,253,301,301a,310,346,442,443a,492a,559a These procedures provide
more rigid fixation for the scaphoid and allow earlier wrist motion.446a A
number of authors have reported their experience with such techniques, but
consensus on the role of screw fixation appears to suggest a definite role for
early internal fixation of the scaphoid.1,110a,121,187,253a,310,389,397,442
Several authors have reported significant problems with screw fixation of acute
scaphoid fractures.1,212,353,389 We reviewed 20 patients with displaced
scaphoid fractures in which open reduction and internal fixation was performed
early, less than 6 weeks. Nineteen of 20 healed. A comminuted fracture had
delayed healing and required a Russe bone graft. Motion and strength were
improved over cast immobilization, and patients returned to work and other
activities by an average of 3 months. Although strong fixation is provided
initially, should fracture union not occur, loosening of the screw and loss of
fixation has been reported. A biomechanical analysis compared the fixation
strength of different bone screws and noted less interfragmentary compression
with the Herbert screw than was anticipated from its unique design of
differential thread-pitch between the distal and proximal screw ends. The
correct application of fracture reduction and alignment devices is essential
for anatomical screw placement.110a The development of cannulated screws placed
over a Kirschner wire or use of intraoperative imaging has improved the
technical factors associated with fracture fixation.70
The current role for compression
screw fixation of scaphoid fractures is limited to displaced fractures,
displaced proximal pole fractures,140 and fracture-dislocations.150 Postfixation
cast immobilization is recommended despite proposals for early motion at 2 to 3
weeks.251 Conclusive studies comparing compression screws with Kirschner wires
or cast immobilization of displaced scaphoid fractures are needed. However, the
role of open reduction and screw fixation is more commonly recommended and
being used.
Scaphoid Nonunion
Treatment
Stable Nonunions
In the treatment
of nonunion of the scaphoid it is essential to maintain the important
principles of fracture healing and at the same time secure correct scaphoid
alignment. Should an asymptomatic patient with scaphoid nonunion have surgical
treatment recommended? Today, more longitudinal or outcome studies do favor
operative intervention to prevent the late sequelae of traumatic arthritis.157a,342,462
Four principles to follow include (1) preservation of blood supply, (2) bone
apposition by inlay graft, (3) internal fixation for fracture stability, and
(4) correction of carpal instability.117,358,400 Failure of scaphoid bone
grafting appears to be associated with inadequate vascularization,
unsatisfactory fracture immobilization, insufficient length of immobilization,
and instability or displacement. A number of questions are currently being
asked regarding the treatment of choice for a nondisplaced scaphoid nonunion.
What is the effect of operative approach on the blood supply? How should
avascular necrosis of the scaphoid be confirmed? Is there a role for electrical
stimulation of nondisplaced scaphoid nonunions? Is internal fixation of the
scaphoid nonunion necessary when the nonunion is not displaced?
Russe Bone Graft. From a survey of
the literature24,156,395 and our experience, it appears that a Rüsse-type inlay
bone graft of the scaphoid is the treatment of choice to which other procedures
should be compared (Fig. 12-98).463,501,506 From a review of four different
treatment options, the volar Russe463 type or dorsal-radial Matti34,351 type
had union rates of 86% and 92%, respectively.117 Studies by others confirm the
excellent results associated with the Russe procedure and report union rates of
85% to 97% for Russe grafting of stable scaphoid nonunions.24,34,155,395 The
need for internal fixation of nondisplaced fractures has been questioned by
some, but one study demonstrated a 97% healing rate after combining a Russe
procedure with internal fixation.
Author's Preferred
Method of Treatment. Our preference and treatment of choice for scaphoid
nonunion is palmar grafting similar to the approach modified by Russe.112 The bone graft is a combination corticocancellous graft.
Russe (as reported by Green has recommended using
a double cortical graft placed side by side (see Fig. 12-98). His technique
emphasized the need to remove the avascular bone and fibrous tissue through a
palmar bone window, thoroughly excavating both the proximal and distal poles
with a curette. We prefer a corticocancellous graft from the iliac crest, which
is inset palmarly and serves to bridge the fracture gap and correct any
displacement or angulation of the scaphoid that has occurred (Fig. 12-99).
Supplemental fixation with a Kirschner wire or wires is preferred.
Postoperative immobilization in a long-arm thumb spica cast is maintained for 6
weeks. The Kirschner wires are removed and a short-arm thumb spica cast is worn
until fracture union is demonstrated on tomography. A radial styloid or radial
metaphysis bone graft can be selected, but the ilium offers a stronger, more
compact, trabecular graft that is easier to sculpt for proper fill.
Vascularized bone grafts from the distal radius (radial artery or distal ulna (ulnar artery)236 have also been
described.
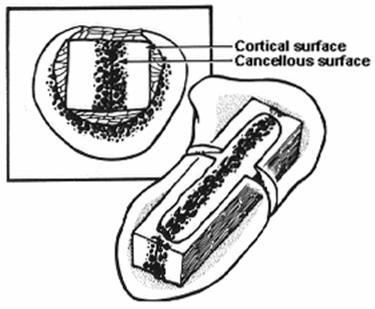
Fig. 12-98 Grefele
osoase Russe. Doua bare corticospongioase
sunt ate in excavatia de la nivelul scafoidului printr-un abord volar. Cavitatea restanta se umple cu bucati de spongie.
Suprafata interioara chiuretata a scafoidului se
inspecteaza pt a evidentia
vascularizatia.
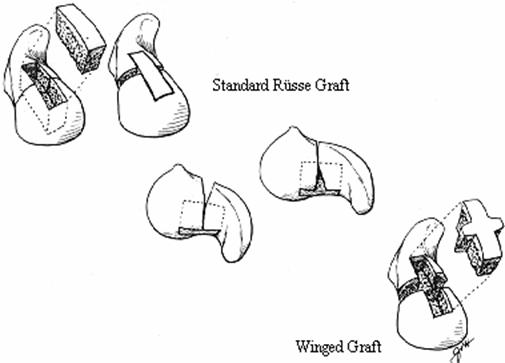
Fig. 12-99 Tehnica Russe originala
consta in impachetarea grefelor cortico-spongioase in jgheabul chiuretat
prin cortexul volar
al ambelor fragmente (stg). Deoarece cortexul volar este
deseori scurtat prin eroziunea fragmentelor este dificila refacrea
lungimii fara introducerea unei grefe corticale (centru). Modificarea
adusa de noi tehnicii originale consta in folosirea unei grefe
cortico-spongioase "cu aripi" recoltata din creasta iliaca care este impactata in jgheabul volar pt a reface lungimea.
The presence of diminished
vascularity of the proximal scaphoid79 is not a contraindication to a palmar
inlay bone graft. If fracture union can be achieved, the relative avascularity
will improve. The time to union is, however, slower, and the rate of nonunion
is increased. Therefore, it is advantageous to confirm avascular necrosis to
determine length and prognosis for successful treatment. Methods of assessing
avascular necrosis include bone scan, tomography, and MRI.175 The latter technique is undoubtedly the most sensitive and
specific. It can provide sequential information on revascularization of the
scaphoid.433a Tomography is a better method of assessing fracture union and may
be just as sensitive and specific in determining avascular changes. The only
definitive test for confirming avascular necrosis, however, is the observation
at surgery of the presence or absence of bleeding from bone. Green231 reported
that when the proximal pole was completely avascular (total lack of bone
bleeding) the likelihood of successful healing with a
graft was virtually nil. If the proximal scaphoid is completely avascular
(Preiser's disease537a), an alternative procedure such as intercarpal
fusion,548 excision of the proximal scaphoid,158 interposition arthroplasty,46
proximal row carpectomy,144a or scaphoid allograft98 should be considered.
Another alternative is some type of vascularized bone graft.562
Electrical
Stimulation. Electrical stimulation (pulsed electromagnetic stimulation
[PEMS]) has been proposed for nondisplaced scaphoid nonunion.5 Studies suggest that it has a role for fractures
3 to 6 months old. In a study of 44 nonunited fractures that were at least 6
months old, union was achieved in 35, combining electrical stimulation and a
thumb spica cast.199 This study and an unpublished
report43 demonstrated better union with a long-arm cast than a short-arm thumb
spica cast. Union rates from these series were 80% and 92%, respectively. The
length of stimulation varied from 8 to 10 hours per day.
The controversy regarding the use of
electrical stimulation in the treatment of scaphoid nonunions, however, remains
unsettled, because there have been no controlled patient series comparing cast
immobilization alone with electrical stimulation in these studies. Its use in
unstable, angulated, displaced nonunions is not indicated. Newer types of
pulsed electromagnetic fields with a shorter stimulation period are now
available (Orthologic Co., Phoenix,
AZ), but there have been no
published reports on their use in treatment of scaphoid nonunions.
Unstable Nonunions
From the work of
Fisk182,183 and later from that of Linscheid and
colleagues,329 instability of the carpus as a result of scaphoid nonunion has
had increased recognition. Displaced scaphoid fractures are more difficult to
diagnose168 and treat, and nonunions of the scaphoid with displacement have a
lower rate of union with an increased potential for radioscaphoid
arthritis.95,117,307,342,462 Techniques to improve scaphoid alignment by palmar
and radiopalmar bone grafting have been developed to correct scaphoid
malalignment18,184 and to restore normal scaphoid length.177,178 A number of
authors have reported their experience with interposition bone grafting for
displaced scaphoid nonunions with internal fixation such as the Herbert
screw,70,121,346 conventional lag screw,178 Enders plate,258a and multiple
Kirschner wires,177 reporting results equal to or superior to the Rüsse
graft.452b Comparative studies on this issue, however, are only a few.405a
Authors' Preferred Method of
Treatment
The indications
for interposition grafting include gross motion at the nonunion site, scaphoid
resorption, and loss of carpal height.184,331 A
dorsal-radial operative approach (Fig. 12-100) can be utilized with Kirschner
wire internal fixation. More commonly, the operative procedure involves an
anterior interposition bone graft, with size based on comparative scaphoid
views of the opposite wrist and intraoperative measurements. An extended palmar
Russe approach between the radial artery and flexor carpi radialis is used to
expose the scaphoid. A gap is noted as the nonunion is debrided. With the two
fragments gently distracted and aligned, reduction is held with a Kirschner
wire. The size of the defect is measured in width and depth, and with an
oscillating saw the exact dimensions of the graft are removed from the iliac
crest. With the graft in place and the scaphoid reduced and held with a
Kirschner wire, a Herbert screw is inserted by the technique described by its
originator (Fig. 12-101). If there is marked DISI angulation of the lunate, it
is best to reduce the lunate and proximal scaphoid by flexing the wrist and
pinning the lunate in a reduced position through the radial styloid first.331 An alternative procedure is to use multiple Kirschner
wires as described by Fernandez (see Fig. 12-89) or dorsal-radial operative
approach (see Fig. 12-100).177 Displaced, small proximal pole fractures are
best approached dorsally.156a,546a
The results of treatment in our
series demonstrated a union rate of 81%, although two cases required a
secondary interposition graft.121 Carpal instability as measured by the
scapholunate angle was corrected from a preoperative mean of 65° to a
postoperative mean of 54°. The capitolunate angle improved from 15° to 3.5°,
and the carpal height ratio improved from 0.51 to postoperative 0.54.
Complications were related to incorrect placement of the Herbert screw and to
resorption of the bone graft. This was usually associated with failure of
healing to the proximal pole. Interposition grafting is preferred when the
palmar gap exceeds 3 mm or more. A modification of the Russe procedure using a
cross-shaped corticocancellous graft or an extended Russe bicortical graft
inserted into the troughs in either pole to prop the scaphoid open for
restoration of length may also be used (see Fig. 12-99). Improved imaging may
provide the technical basis for more accurate bone graft configuration,
scaphoid reconstruction, and internal fixation, making interposition grafting
more practical and easier for the surgeon.45a,405b
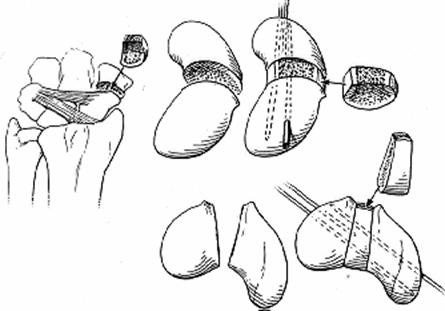
Fig.
12-100
A radial approach with partial
radial styloidectomy may be indicated in patients with a severe humpback
scaphoid deformity, to judge the necessary degree of corrective realignment.
The dorsal osteophyte of the humpback should be excised to assist in the
reduction. This procedure should be chosen with caution, because the
traditional Matti-Russe graft has a superior union rate and is capable of
correcting mild carpal instability. The Russe technique remains the gold
standard to which other scaphoid grafting procedures must be compared.
It may be difficult to completely
correct carpal instability in long-standing cases, and these patients may be
better served by various salvage procedures.
Vascularized Bone
Graft. A vascularized bone graft to the scaphoid562 for established
nonunion is recommended for (1) avascular necrosis, (2) failed bone grafting
procedure (eg, failed Russe or interposition graft), and (3) Preiser's disease.
The vascular bone graft can be harvested from the distal radius (second dorsal
compartment) or from the second metacarpal. A dorsal-radial approach is
required (Fig. 12-102). We recommend harvesting the vascular graft first from
the radius, using loop magnification. The radial artery branches are then
dissected and followed to the radius. The rectangular bone graft is then
harvested with great care taken to protect the vascular pedicle. The scaphoid
is approached dorsoradially, and the nonunion site is excavated. Kirschner
wires are positioned by retrograde insertion and then the vascularized bone
graft is inserted. With the graft in place, the Kirschner wires are drilled
across the nonunion site. A radial styloidectomy may be required because the
breadth (width) of the scaphoid is usually increased.
For avascular necrosis of the
scaphoid, one must remove all of the avascular bone (usually proximal third).
The vascular graft is inlaid with care taken to protect the pedicle, and
additional cancellous bone may be packed around the vascular graft. Kirschner
wire fixation is used if the scaphoid appears unstable. For a failed primary
bone graft, the previous graft fragments must be removed and a fresh surface
created between the ends of each fragment. The vascular graft is inserted
usually as an inlay graft or alternatively as an interposition graft. Kirschner
wire or compression screw fixation is usually recommended. Cast immobilization
is continued until tomograms show solid healing.
For Preiser's disease537a (avascular
necrosis of the entire scaphoid), a vascularized bone graft is the procedure of
choice if nonoperative methods (splint, rest, electrical stimulation) fail to
resolve the problem. If the scaphoid begins to show collapse similar to that
seen in a nonunion, bone grafting (preferably a vascularized graft from the
distal radius) is recommended. The technique is similar to that described in
the preceding paragraph except that the entire scaphoid is excavated of
avascular bone. Cast immobilization is recommended as with a fracture nonunion.
Long-term splint protection may be needed for up to 6 months because
revascularization is a slow process in Preiser's disease.
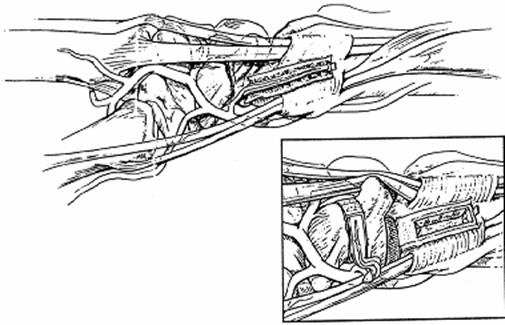
Fig.
12-102

